

Abstract
Introduction
Autologous T cells expressing a CD19-specific chimeric antigen receptor (CAR) have produced impressive minimal residual disease-negative complete remission (MRD-neg CR) rates in relapsed/refractory B-cell acute lymphoblastic leukemia (B-ALL) patients (pts). Factors associated with durable remission in pts achieving MRD-neg CR after immunotherapy with T cells engineered with a CD19 CAR (FMC63.41bb.3ζ) have not been elucidated.
Methods
We studied factors impacting disease-free survival (DFS) of adults with B-ALL treated with lymphodepletion chemotherapy and CD19 CAR-T cells in a phase I/II clinical trial (NCT01865617). Pts were eligible for this analysis if they had bone marrow leukemia identified by flow cytometry and/or extramedullary disease before CAR-T cell therapy, and received CAR-T cells at or below the previously determined maximum tolerated dose (MTD; Turtle, JCI 2016). Anti-tumor response after CAR-T cell infusion was assessed by bone marrow aspiration and biopsy, with PET-CT performed in pts with extramedullary disease. High resolution (1:10,000) flow cytometry was used to identify marrow MRD, and marrow from pts in MRD-neg CR was evaluated by high throughput sequencing (HTS) of IGH, IGK, TRB, TRD, and TRG genes. Cox regression univariate and stepwise multivariable modeling were performed to identify factors associated with DFS.
Results
Of 57 pts who received lymphodepletion and CD19 CAR-T cells, 53 were evaluable for response and 4 were not evaluable (one MRD-neg CR before CAR-T cell infusion; 2 received CAR-T cells above the MTD; one fatal neurotoxicity prior to restaging).
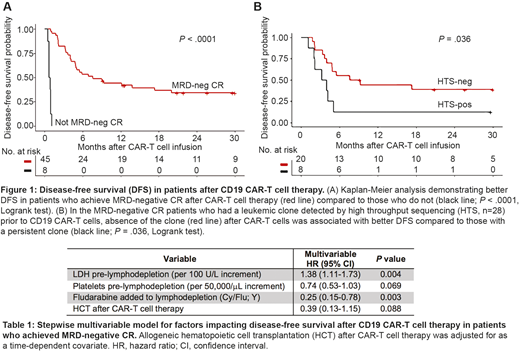
Forty-five of 53 restaged pts (85%) achieved MRD-neg CR after CAR-T cell therapy. With a median follow-up of 30.9 months, DFS and overall survival (OS) were longer in pts who achieved MRD-neg CR compared to those who did not (Fig 1A; median DFS, 7.6 vs 0.8 months, P < .0001; median OS, 20.0 vs 5.0 months, P = .014). Twenty-eight of the 45 pts who achieved MRD-neg CR had a leukemic clone identified by HTS prior to CAR-T cell infusion, and in 20 of these pts (71%), the leukemic clone was not detected in marrow 3 weeks after CAR-T cell infusion. DFS was better in MRD-neg CR pts with no detected malignant clone compared to those with a persistent clone by HTS (Fig 1B; median DFS, 8.4 vs 3.6 months, P = .036).
We then used stepwise multivariable modeling to determine factors impacting DFS in the pts who achieved MRD-neg CR (n = 45). Better DFS was seen in pts with a higher pre-lymphodepletion platelet count (hazard ratio, HR 0.65 [95% CI; 0.47-0.88] per 50,000/μL increment P = .006), lower pre-lymphodepletion LDH (HR 1.39 [1.12-1.74] per 100 U/L increment, P = .003), and with incorporation of fludarabine into the cyclophosphamide-based lymphodepletion (Cy/Flu; HR 0.34 [0.15-0.78], P = .011). Similar findings were noted in analysis of MRD-neg CR pts who had no malignant clone by HTS after CAR-T cells. Pts with platelets ≥100,000/μL and normal LDH before lymphodepletion who received Cy/Flu (good risk, n = 15) had 2-year point estimates of DFS and OS of 78% and 86%, respectively.
Allogeneic hematopoietic cell transplantation (HCT) is standard of care in suitable R/R adult B-ALL pts after achieving MRD-neg CR. Eighteen pts in MRD-neg CR after CAR-T cells underwent HCT a median of 2.3 months after CAR-T cell infusion. We analyzed the effect on DFS of HCT after CAR-T cell therapy by treating HCT as a time-dependent covariate. After adjusting for LDH, platelets, and Cy/Flu lymphodepletion, pts undergoing HCT after CAR-T cell therapy had lower risk of failure for DFS compared to those who did not undergo HCT (Table 1). No significant interaction effect was seen between HCT and risk group (P = .51). With a median follow-up of 28.4 months after HCT, 2-year point estimates of DFS and OS were 61% and 72% respectively. The 2-year cumulative incidence of relapse was 17% and non-relapse mortality was 23%.
Conclusion
A high rate of MRD-neg CR was seen following CD19 CAR-T cell therapy in adult B-ALL pts and is associated with improved DFS and OS. Absence of the index clone by HTS after CAR-T cells was associated with better DFS, suggesting deeper responses are associated with improved outcomes. Stepwise multivariable modeling identifies better DFS in pts with higher pre-lymphodepletion platelet count and lower LDH, and with use of Cy/Flu lymphodepletion. After adjusting for these factors, HCT after CD19 CAR-T cells may also be associated with better DFS.
Hay:DAVA Oncology: Honoraria. Hirayama:DAVA Oncology: Honoraria. Li:Juno Therapeutics: Employment, Equity Ownership. Till:Mustang Bio: Patents & Royalties, Research Funding. Kiem:Rocket Pharmaceuticals: Consultancy; Homology Medicine: Consultancy; Magenta: Consultancy. Ramos:Seattle Genetics: Employment, Equity Ownership. Shadman:Qilu Puget Sound Biotherapeutics: Consultancy; AstraZeneca: Consultancy; Pharmacyclics: Research Funding; Genentech: Consultancy; Mustang Biopharma: Research Funding; AbbVie: Consultancy; Celgene: Research Funding; Verastem: Consultancy; Acerta Pharma: Research Funding; Genentech: Research Funding; TG Therapeutics: Research Funding; Beigene: Research Funding; Gilead Sciences: Research Funding. Cassaday:Adaptive Biotechnologies: Consultancy; Amgen: Consultancy, Research Funding; Incyte: Research Funding; Seattle Genetics: Other: Spouse Employment, Research Funding; Jazz Pharmaceuticals: Consultancy; Kite Pharma: Research Funding; Pfizer: Consultancy, Research Funding; Merck: Research Funding. Acharya:Juno Therapeutics: Research Funding; Teva: Honoraria. Riddell:Adaptive Biotechnologies: Consultancy; NOHLA: Consultancy; Juno Therapeutics: Equity Ownership, Patents & Royalties, Research Funding; Cell Medica: Membership on an entity's Board of Directors or advisory committees. Maloney:Seattle Genetics: Honoraria; Roche/Genentech: Honoraria; GlaxoSmithKline: Research Funding; Janssen Scientific Affairs: Honoraria; Juno Therapeutics: Research Funding. Turtle:Adaptive Biotechnologies: Consultancy; Eureka Therapeutics: Equity Ownership, Membership on an entity's Board of Directors or advisory committees; Juno Therapeutics / Celgene: Consultancy, Patents & Royalties, Research Funding; Gilead: Consultancy; Nektar Therapeutics: Consultancy, Research Funding; Caribou Biosciences: Consultancy; Precision Biosciences: Equity Ownership, Membership on an entity's Board of Directors or advisory committees; Bluebird Bio: Consultancy; Aptevo: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal